
The most important motor tract which includes the Lateral and Anterior Corticospinal tract. Note there are no particular first, second order neurones that are consistent with the ascending tracts.
The guide to ascertaining weakness depends on the motor pathway that runs from the motor cortex in the frontal cortex (pre-central gyrus/motor strip) to the muscle.
In order to determine where the lesion is (mostly Neurologists do this) but it is good to have an understanding of the motor pathway because in an exam setting it is useful. You will often encounter the term weak. My guide to determine whether a patient is weak is to determine does this patient have UMN or LMN weakness. With the advent of radiology we can predict the type of signs but for the purpose of this website we will work things out from basic principles.
UMN Weakness
Firstly we need to know the pathway of the corticospinal tract.

Primary motor cortex is located in the pre-central gyrus. The fibers descend through the internal capsule, cerebral peduncles, and decussate at the level of the pyramids before synapsing at the level of the anterior horn of the spinal cord.
Lesions at the cortex: will produce contra-lateral weakness
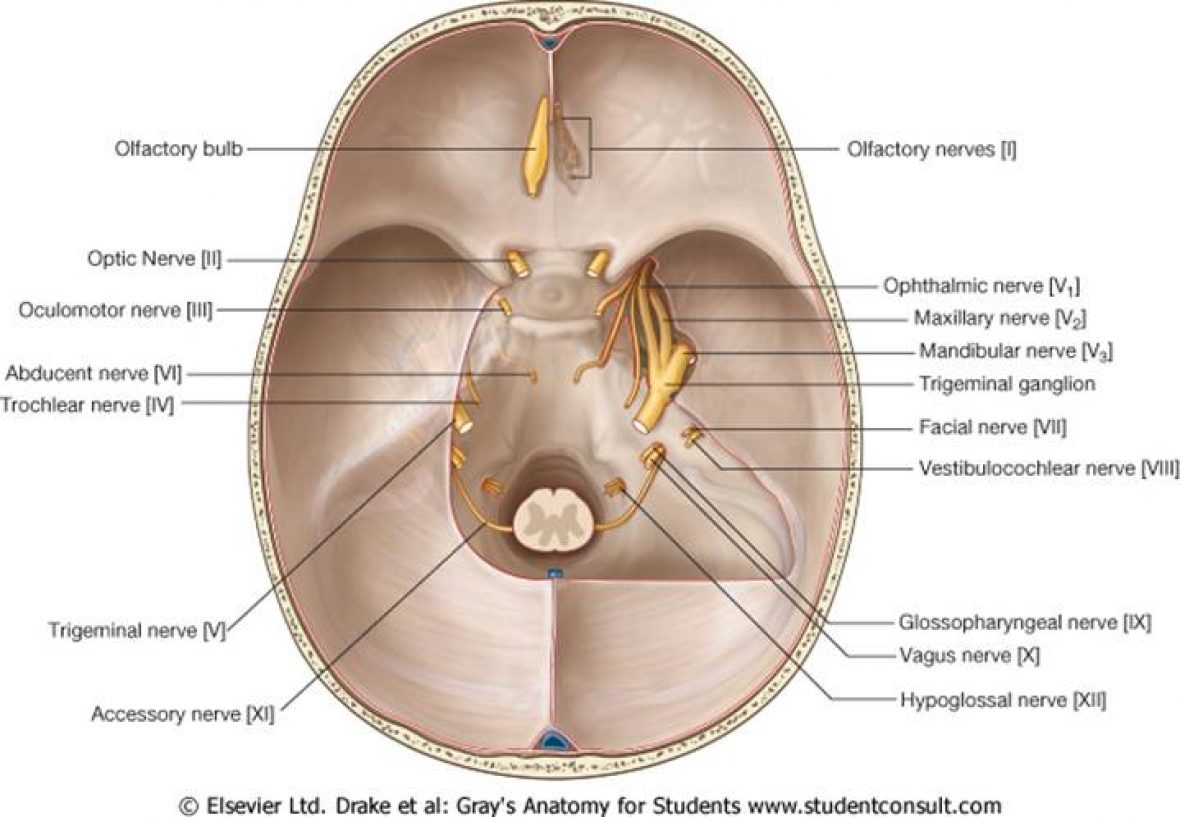
Lesions in the brainstem: depending on the type of pathology will cause hemiplegia, quadriplegia WITH associated cranial nerve symptoms.
Cord lesions produce LMN weakness at the level of the spinal cord but UMN lesions below the level.
UMN Signs:
- Hypertonia- Clasp Knife rigidity
- Hypereflexia
- +ve Babinski’s sign
- +ve Hofmans sign (upper limb equivalent)
- Note in the Upper Limb flexors>>extensors
- Note in the Lower Limb extensors>flexors
- Clonus
LMN Weakness
The lower motor neurone pathway will run all the way from the anterior horn cell, plexus, nerve root, nerve itself, neuro-muscular junction and finally the muscle
Neurosurgeons would be more interested in nerve root, brachial plexus pathology rather than that of the rest which can be managed by the medical team. Yes myopathies are investigated by neurosurgeons by muscle biopsies.
Nerve root problems will generally produce a motor or sensory problem indicated by their myotomal and dermatomal distribution. Knowledge of these dermatomes and myotomes are important in patients with disc herniations as they can provide a reasonable estimation to the location of the pathology
LMNeurone Signs:
Hypotonia
Hyporeflexia
Flaccid Paralysis
Fasiculations